医影在线
标题: V0154:右上纵膈局限性巨淋巴结增生(透明血管型) [打印本页]
作者: pp 时间: 2006-12-15 04:38
标题: V0154:右上纵膈局限性巨淋巴结增生(透明血管型)
由caihe版主提供讨论的类似病例连接:
http://www.radida.com/bbs/forum.php?mod=viewthread&tid=17582
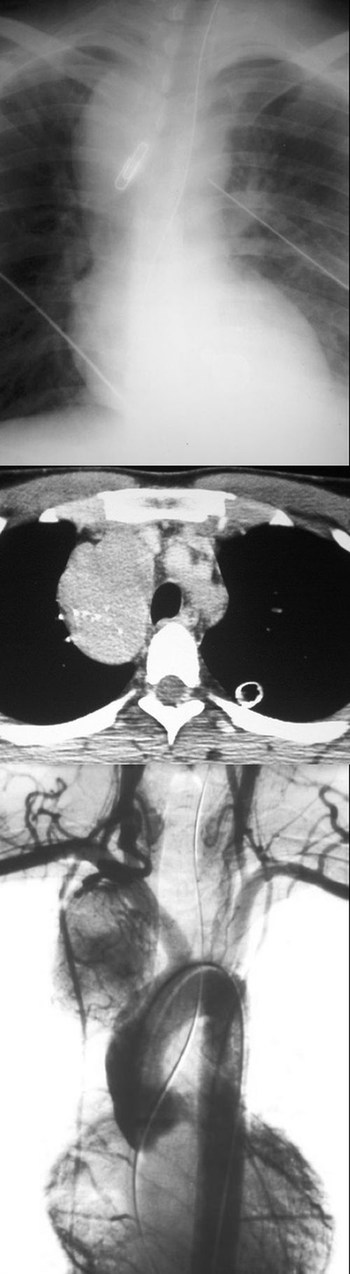
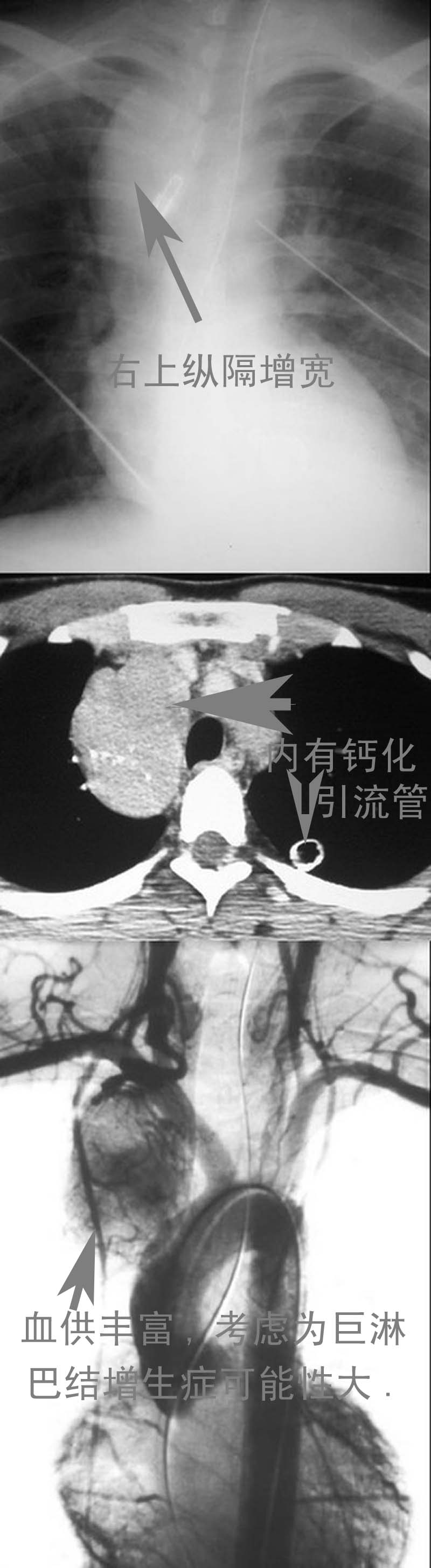
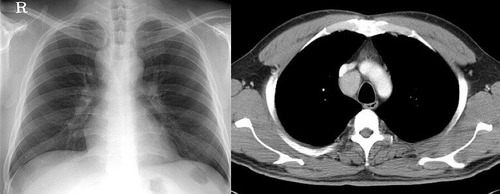
男性,26岁。右上胸部外伤急诊患者。平片发现右上纵膈异常而行ct和dsa检查。
[本贴已被 向医生 于 2008-12-9 23:12:20 修改过]
作者: dyqct 时间: 2006-12-16 03:28
标题: 占位性病变
占位性病变
[本贴已被 dyqct 于 2006-12-15 19:29:17 修改过]
作者: 卜一 时间: 2006-12-16 14:25
定位:中纵隔.
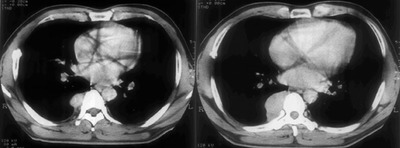
特征:类圆形,边界清楚,占位效应明显,富血供.
定性:首先考虑_淋巴瘤.
建议:增强.
作者: ssm999 时间: 2006-12-17 04:29
畸胎瘤
作者: 漫步云端 时间: 2006-12-18 05:44
中纵隔.类圆形,边界清楚,占位效应明显,富血供,良性病变可能性大。
作者: pp 时间: 2006-12-25 00:39
标题: 公布病理结果
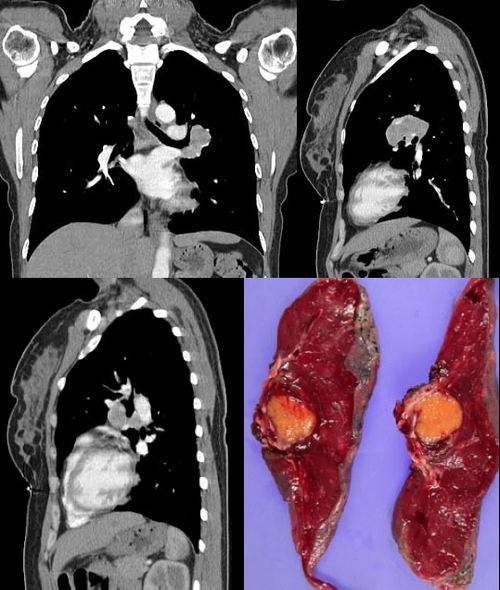
局限性巨淋巴结增生(透明血管型)。
]

请看由zhangyong版主发布的腹膜后局限性巨淋巴结增生病例:
v0090:http://www.radida.com/radinet/read.php?tid=15905
病例①:
age/sex: 58/m
chief complaints: extremity weakness, sensory change, and skin lesion
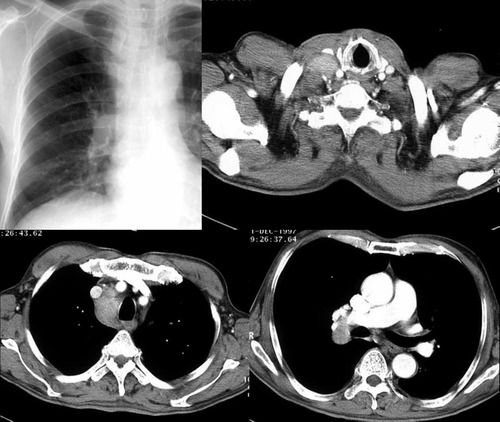
病例②:
age / sex:40 / m
chief complaint:routine check-up . history of operation due to mediastinal mass
ten years before.

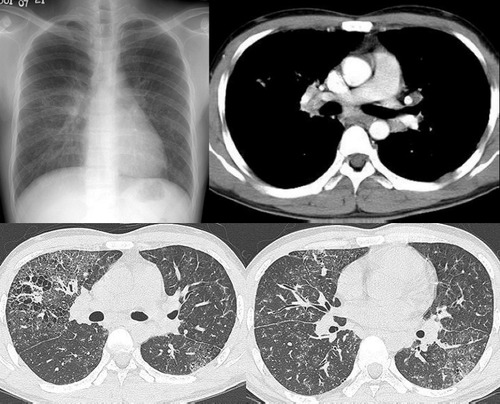
病例③:
age / sex:23 / male
chief complaint: recurrent lymphadenopathy in the preauricular,
elbow and bilateral inguinal areas
diagnosis: multicentric castleman';s disease with lung involvement
(lymphocytic interstitial pneumonitis)
病例④:
age / sex:44 / female
chief complaint: asymptomatic, chest radiograph abnormality
病例⑤:
age / sex:21 / male
chief complaint:incidental detected mass at left hilum

病例⑥:
age / sex:31 / f
chief complaint:incidental cxr abnormality on routine health exam

病例⑦:
age / sex:40 / m
chief complaint: incidental abnormality on chest radiograph

病例⑧:
39 / m; chest discomfort
病例⑨:
40 / f, incidental mass on croutine check

病例⑩:
age / sex:28 / f
chief complaint: left hilar abnormality on routine chest radiograph
[本贴已被 pp 于 2006-12-24 17:07:30 修改过]
作者: pp 时间: 2006-12-25 00:50
标题: 讨论:
brief review
castleman disease, also known as angiofollicular hyperplasia
or giant lymph node hyperplasia, is a rare disorder of lymphoid tissue.
unclear etiology and pathogenesis. this disease may occur anywhere
along the lymphatic chain but it is most commonly found as a solitary mass
in the mediastinum. two distinct histologic patterns of castleman disease
have been described, including the hyaline-vascular type,
accounting for 90% of cases, and the remainder of cases as the plasma cell type,
which is often associated with constitutional symptoms. three patterns have
been reported on ct or mri, including a solitary noninvasive mass (50%),
a dominant infiltrative mass with associated lymphadenopathy (40%),
and a matted lymphadenopathy without a dominant mass (10%)
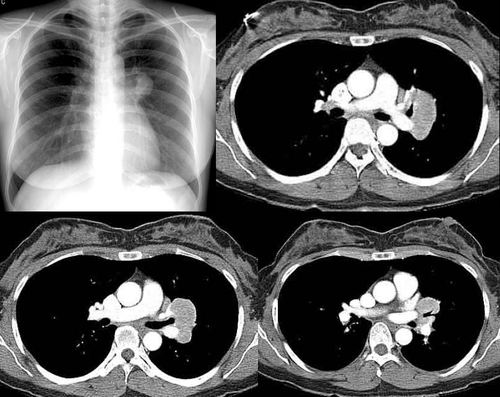
in castleman disease, ct with contrast material usually shows a dense
uniform enhancement. dynamic ct demonstrates early rapid enhancement
and washout in the delayed phase, which are considered as typical imaging
characteristics that help to differentiate this disease from other mediastinal tumors
such as lymphoma etc. furthermore, peripheral hypervascularity is a characteristic
finding on power doppler ultrasonography. a punctate or arborizing pattern of
calcification may be seen. some recent studies have reported a considerable
number of cases showing heterogeneous attenuation. meador and mclarney reported
that tumors greater than 5 cm in diameter generally demonstrate heterogeneous
enhancement. in several studies, a focal low attenuation area within the mass
showing delayed enhancement on dynamic ct or mri, was pathologically proven
to be central stellate fibrosis interspersed within the mass. an mri study has
been reported to be useful for the evaluation of peripheral or tumoral hypervascularity
and the relationship with adjacent vascular structures, because vascular structures
appear signal void with high contrast to the mass.
treatment of castleman disease is as follows. surgical resection is recommended
for patients with the unicentric variant of cd because surgical removal of a unicentric
mass of hyaline-vascular or hyaline-vascular/plasma cell type is curative.
but if it is not possible, partial resection, radiotherapy, or observation alone may
be helpful instead of excessively aggressivie therapy.
patients with multicentric disease, either hyaline-vascular or plasma cell type,
do not benefit from surgical management and should be candidates
for multimodality therapy, the nature of which has yet to be defined..
作者: dyqct 时间: 2006-12-25 01:06
结果收到,谢谢楼主。
作者: zyx168 时间: 2006-12-25 18:19
标题: 回复:v0154:右上纵膈局限性巨淋巴结增生(透明血管型)
结果收到,谢谢版主。
作者: 李晓阳 时间: 2007-7-3 04:01
学习了
作者: pujunzhi 时间: 2012-6-23 10:13
v0154:右上纵膈局限性巨淋巴结增生(透明血管型)
结果收到,谢谢版主。
作者: shibing 时间: 2012-8-14 07:25
局限性巨淋巴结增生
| 欢迎光临 医影在线 (http://bbs.radida.com/bbs/) |
Powered by Discuz! X3.2 |